

The Incentive Fix That Could Cut Your Medical Bill
New AER Paper finds....

We usually assume something simple about health care: when doctors have a financial stake in something, costs go up.
It sounds intuitive. More ownership. More profit motive. More opportunities for doctors to prescribe procedures that patients don’t need.
But what if the opposite can happen?
A new paper by Decode Econ Educator Network member Beth Munnich (University of Louisville) and her coauthors, published in the American Economic Review, finds that when physicians become owners of ambulatory surgery centers, Medicare spending tied to those physicians actually falls — in some cases dramatically. Saving patients and taxpayers a lot of money.
To understand why, we need to revisit one of the most important ideas in economics.
The Agency Problem in Health Care
The principal–agent problem happens when someone makes decisions on your behalf but does not fully bear the consequences of those decisions.
Health care is full of these tensions. Doctors decide where your procedure happens. You or Medicare pays the bill. Yet physicians often do not face the same financial tradeoffs that patients or taxpayers do.
Consider same-day outpatient procedures such as colonoscopies, orthopedic surgeries, or eye procedures. They can be performed in either a hospital outpatient department (HOPD) or an ambulatory surgery center (ASC). Hospitals are typically much more expensive for the exact same procedure. Medicare might pay substantially more in a hospital setting than in a surgery center, even when the physician and the procedure are identical.
However, physicians are paid the same professional fee regardless of where the procedure takes place. From the doctor’s perspective, there is no direct financial incentive to choose the lower-cost setting.
That is the agency problem in action.
What Changes When Doctors Become Owners
Ambulatory surgery centers are often privately owned, and physicians can buy equity stakes in them. When physicians become owners, they become residual claimants on the facility’s profits. Ownership introduces a new incentive to shift procedures into the surgery center setting.
The authors use Medicare fee-for-service data from 2013 to 2019 and a difference-in-differences design to examine what happens when physicians acquire ownership stakes. The obvious concern is that financial incentives might distort care. Do doctors oversupply procedures? Do they inappropriately steer patients? Do costs rise?
The Results are Striking
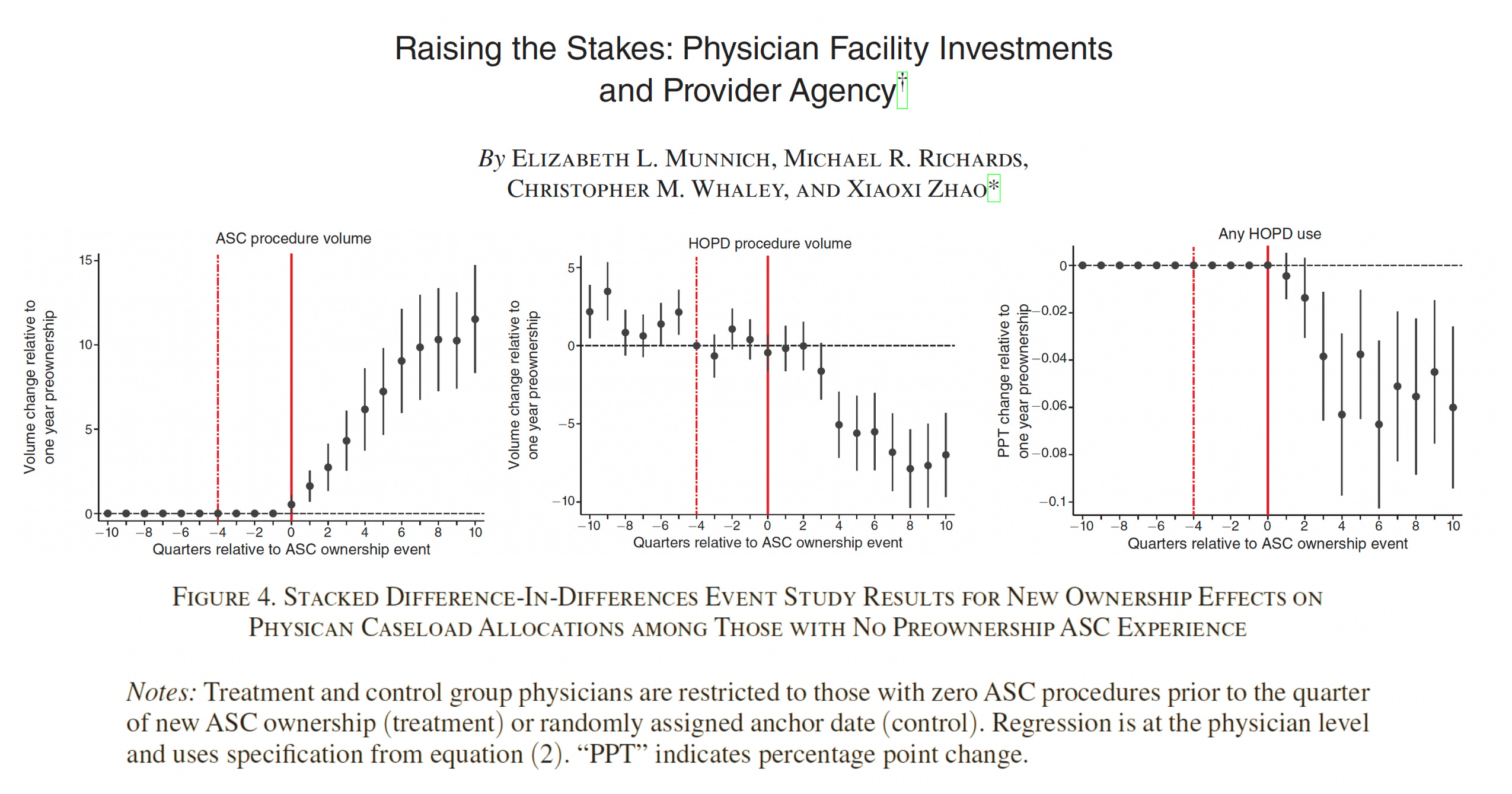
Physicians shift procedures to ambulatory surgery centers after becoming owners. However, the effects differ depending on prior experience. Physicians who were already using surgery centers increase ASC volume by roughly 15 to 20 percent and reduce hospital-based procedures modestly. Their total procedure volume rises slightly, yet Medicare spending tied to their patients falls by about 11 percent.
The most dramatic changes occur among physicians who had never used surgery centers before becoming owners. These physicians shift procedures almost one-for-one from hospitals into ASCs. Between one-third and one-half of their Medicare cases move to the lower-cost setting. Within a year, they are 5 to 6 percent less likely to use hospital outpatient departments. As a result, Medicare spending associated with these physicians falls by roughly 40 percent.
Did Quality Suffer?
Importantly, these savings are not driven by treating less medically complex patients or cutting corners. The reductions are not explained by changes in case complexity, and there is no clear evidence of declining quality. Emergency department visits do not increase. There is little indication of strategic patient selection.
In other words, physicians are not gaming the system. They are reallocating procedures to a more efficient setting.
The Bottomline
The broader insight is subtle but important. Physicians may underutilize ambulatory surgery centers when they lack explicit incentives to use them. This does not imply bad intent. It reflects imperfect agency. When incentives are misaligned, physicians may not fully internalize the financial burden placed on patients and payers. When ownership better aligns those interests, behavior changes.
We often assume that financial incentives in medicine are inherently dangerous. This paper offers a more nuanced view. Misaligned incentives can produce inefficiencies, but well-aligned incentives can reduce costs without compromising care.
In this case, physician entrepreneurship appears to mitigate the principal–agent problem rather than exacerbate it.
Citation
Munnich, E. L., Richards, M. R., Whaley, C. M., & Zhao, X. (2026). Raising the Stakes: Physician Facility Investments and Provider Agency. American Economic Review, 116(2), 502-534.
Thank you for this awesome write-up! It was a fun paper to work on.
Thanks for sharing this summary, Dr. A!